The Mako Difference
Mako Partial Knee can help lead to better outcomes, like less pain and shorter recovery times2, compared to manual surgery.
In clinical studies, compared to manual partial knee replacement surgery, Mako Partial Knee demonstrated:
-
More accurate bone removal, which may result in improved outcomes and functioning of the knee.1,2
-
Less pain in the days and weeks following surgery.2,3
-
Shorter hospital stay.2
-
Quicker recovery, where 9 out of 10 patients were walking without an aid, such as a cane or walker, three weeks after surgery.4
-
91% of patients being satisfied or very satisfied five years after surgery, and 92% satisfied or very satisfied ten years after surgery.5,6
Learn more about Mako Robotic-Arm assisted surgery.
Discover Mako SmartRobotics™ surgeons near you to see if a Mako Knee procedure is an option for you.
The journey of Mako Partial Knee Replacement (PKA) surgery
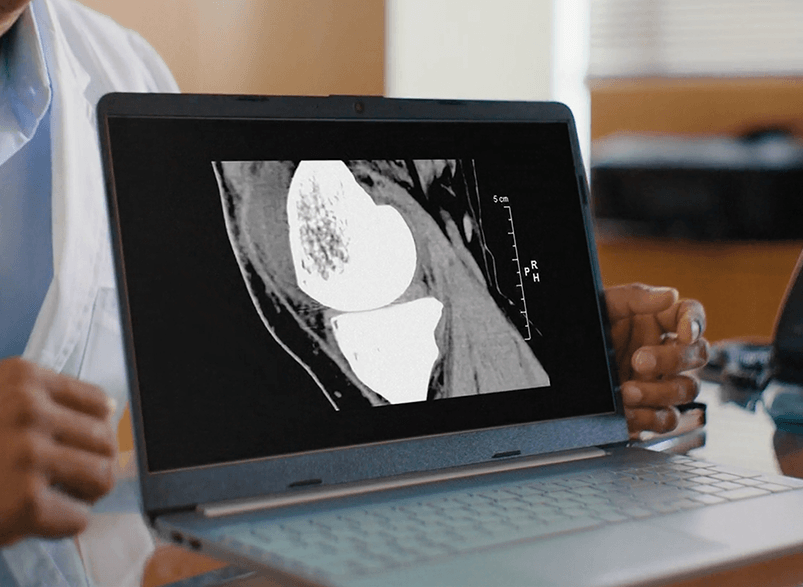
Step 1 - Scan
Before surgery, a CT scan of your knee is taken and used to develop a 3D virtual model of your unique joint.
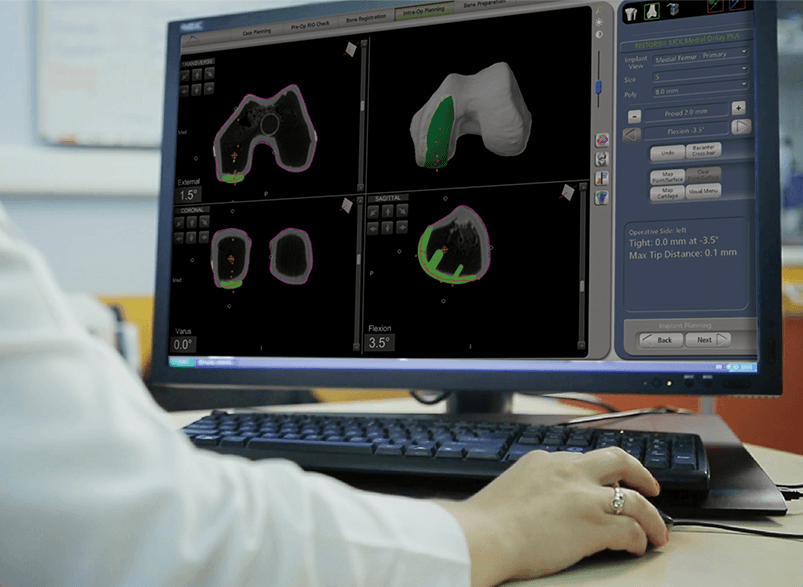
Step 2 - Plan
The second step is patient-specific surgical planning.
Your doctor uses the 3D CT-based model to evaluate your bone structure, disease severity, joint alignment and even the surrounding bone and tissue so that they can determine the desired size, placement and alignment of your implant.
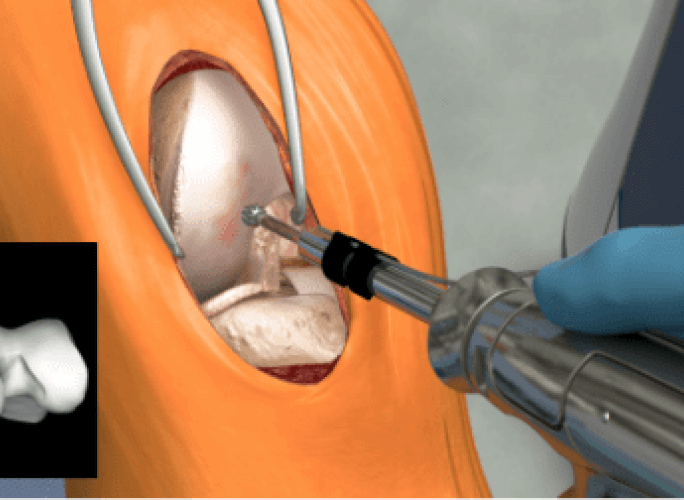
Step 3 - Mako Can
In the operating room, your surgeon guides Mako’s robotic arm to remove arthritic bone and cartilage from the knee.
Mako’s Accustop™ technology creates a virtual boundary that provides tactile resistance to help the surgeon stay within the boundaries defined in your surgical plan.
Throughout the procedure, Mako provides real-time data to your surgeon, allowing them to assess the movement and tension of your joint and adjust your surgical plan if desired.
Is Mako right for me?
Mako Partial Knee is for people who:
-
Experience severe knee pain or stiffness resulting from: noninflammatory degenerative joint disease (including osteoarthritis, traumatic arthritis, or avascular necrosis), rheumatoid arthritis or post-traumatic arthritis.
-
Haven’t experienced adequate relief with conservative treatment options, like bracing, medication or joint fluid supplements.
-
Have early to mid-stage osteoarthritis that doesn’t affect all 3 compartments of the knee.